On Monday the Washington Post published a propaganda piece by Rwandan Minister of Health Agnes Binagwahois. She talks writes of “an opportunity to lay the foundation for an AIDS-free generation,” which inevitably means a primary focus on “voluntary, adult” male circumcision. It’s a matter of faith that this will solve everything, and as a result, there must not be any ethical issues to discuss. Anyway, they’re only implementing “voluntary, adult” male circumcision. Just believe.
Experience demands a closer inquiry. When public health officials speak of “voluntary, adult” male circumcision, they never mean voluntary or adult. They say it, as Binagwahois does. That phrase is mandatory. They do mandatory very well.
We have the capacity to save nearly 4 million lives in sub-Saharan Africa, the hardest hit region in the world, by scaling up voluntary medical male circumcision — the best tool we have for HIV prevention. But the only method widely approved for funding is the surgical method, which is expensive and impractical for countries lacking physicians and surgical infrastructure.
She didn’t say adult yet, but that shows up. She writes that “[p]ublic health officials set a goal to reach nearly 20 million men ages 15 to 49 by 2015…”. I’d quibble over a 15-year-old being an adult, but I also think a 15-year-old is capable of informed consent. If only her statement were true.
In the essay she links to a paper outlining Rwanda’s “national goal”, which can be summed up as a willful violation of human rights. From page 61:
High coverage of male circumcision has been shown to be effective in reducing heterosexual transmission of HIV infection. Under this Outcome, circumcision will be promoted to adult males, with the aim of increasing the prevalence of circumcision. In addition, although circumcision of newborn boys will not contribute to the result of reduced sexual transmission of HIV during the period covered by this NSP, it is nonetheless an important long-term strategy for reducing susceptibility to HIV infection in the Rwandan population.
In case it isn’t quite clear enough, the report includes this table:
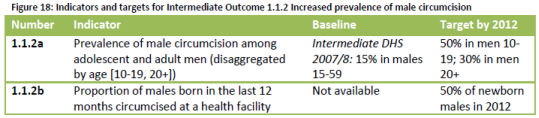
Then it’s summarized:
Output 1.1.2.1. Newborn boys, adolescents and adults have increased access to circumcision
Key strategies:
- i. Advocacy for integration of circumcision in minimum package of health centers
- ii. Promotion and provision of male circumcision for adolescents and adults
- iii. Promotion and provision of male circumcision for newborn boys
She also links to the WHO’s 2011 revised report, Progress in scale-up of male circumcision for HIV prevention in Eastern and Southern Africa: Focus on service delivery. On page 14 the WHO describes Rwanda’s current “Service” delivery strategy.
Plans include the integration of MC into existing services with campaigns and mobile services to increase coverage. Service delivery has begun at selected sites, including military settings. Neonatal and adolescent MC is articulated in the longer-term plan.
About that “long-term” plan. Rwanda keeps saying “long-term”, but a close look at Figure 18 shows its definition. Rwanda’s target for 2012 is 50% of all newborn males. Rwanda is actively circumcising newborn males now. The limitation is clearly not intent. I believe they are sincere in focusing on adults, although less so on the “voluntary” aspect. But it’s obvious where the real focus is. Fear of HIV in the presence of effective-but-elective non-surgical interventions leads to a blatant disregard for the rights of children. It is disgusting.
Since there is a national plan to circumcise newborn and adolescent males without their consent, why does Binagwahois not say so explicitly? Instead, she pretends that the current focus is only on adults and limits herself to advertising for the “non-surgical” PrePex device. Since she doesn’t know the meaning of voluntary or adult, it isn’t particularly surprising that she doesn’t understand the definition of surgery. The ability to limit bleeding does not mean it is non-surgical. Condoms are non-surgical. Foreskin removal is surgical. It’s not refuted just because the device’s manufacturer says so. Regurgitating marketing material is not supposed to be the job of a public health official.
For consideration relevant to the ethics and practicality of the PrePex rollout, Figure 6 in the study (NSFW) Binagwahois’ essay links suggests to me that there will be complications when use of this device is scaled to 20 million men in field settings. And to be fair to Circ MedTech, it promotes PrePex for adult male circumcision. We’ll see if their focus remains on voluntary, adult male circumcision.