It takes a special commitment to ignorance to cherry-pick evidence to prove that opponents cherry-pick evidence. Mark Joseph Stern possesses that special commitment.
There are facts about circumcision—but you won’t find them easily on the Internet. Parents looking for straightforward evidence about benefits and risks are less likely to stumble across the Centers for Disease Control and Prevention than Intact America, which confronts viewers with a screaming, bloodied infant and demands that hospitals “stop experimenting on baby boys.†Just a quick Google search away lies the Circumcision Complex, a website that speculates that circumcision leads to Oedipus and castration complexes, to say nothing of the practice’s alleged brutal physiological harms. If you do locate the rare rational and informed circumcision article, you’ll be assaulted by a vitriolic mob of commenters accusing the author of encouraging “genital mutilation.â€
One paragraph in, and there’s so much to unpack. First, the obvious point is that Mr. Stern is another in a long line of lazy writers who thinks that the ability to type a word into Google proves much of anything for a story. If it’s just “a quick Google search away”, in a paragraph filled with links, it’s reasonable to expect an author to include the search he used to get to the evidence of alleged malfeasance. When I use Google to search circumcision, I get Wikiepdia, news articles, KidsHealth.org, the Mayo Clinic, the government’s Medline Plus, Intact America, Jewish Virtual Library, NOCIRC, and so on. I’ll point out that only the results for Intact America and NOCIRC are to something decidedly against non-therapeutic child circumcision, but so what? It’s a search algorithm. That’s easily gamed. It doesn’t prove Mr. Stern’s silly angle.
That “rare rational and informed circumcision article” is another in Hanna Rosin’s string of awful circumcision defenses.
As for the vitriol, this is the internet. Never read the comments. That doesn’t excuse the comments. They’re often offensive and uninformed and the people who engage in that behavior are wrong, even if they’re ostensibly on my side. But you’ll find them on both sides. It doesn’t prove anything on the argument. Using it as evidence against the argument is ad hominem.
So. There are facts about circumcision. Circumcision is the “surgical removal of the foreskin of males”. The foreskin is the “loose fold of skin that covers the glans of the penis”. Those are facts. But he’s implying the context of non-therapeutic male child circumcision. What should parents want?
Parents shouldn’t want anything, of course, because this is not their decision. Just like we don’t allow them to cut off any other normal body parts of their children, they do not possess a right to circumcise their sons for any reason other than immediate medical need that can’t be adequately resolved with less-invasive methods. Proxy consent is not sufficient for non-theratpeutic circumcision. But because our society doesn’t yet grasp the full implication of an equal right to bodily integrity, parents want information. Fortunately, there is scientific evidence against non-therapeutic circumcision!
The normal, healthy foreskin is normal and healthy. If parents leave it alone, as they should, statistics demonstrate that their son(s) will almost never need any intervention for his foreskin, and much less a medically-necessary circumcision.
Of every 1,000 boys who are circumcised:
- 20 to 30 will have a surgical complication, such as too much bleeding or infection in the area.
- 2 to 3 will have a more serious complication that needs more treatment. Examples include having too much skin removed or more serious bleeding.
- 2 will be admitted to hospital for a urinary tract infection (UTI) before they are one year old.
- About 10 babies may need to have the circumcision done again because of a poor result.
In rare cases, pain relief methods and medicines can cause side effects and complications. You should talk to your baby’s doctor about the possible risks.
Of every 1,000 boys who *are not* circumcised:
- 7 will be admitted to hospital for a UTI before they are one year old.
- 10 will have a circumcision later in life for medical reasons, such as a condition called phimosis. Phimosis is when the opening of the foreskin is scarred and narrow because of infections in the area that keep coming back. Older children who are circumcised may need a general anesthetic, and may have more complications than newborns.
Those numbers, from the Canadian Pediatric Society, are hardly compelling in favor of circumcising healthy children. Non-therapeutic circumcision prevents 5 boys (0.5%) from being admitted to a hospital with a UTI in the first year of life. Yet, between 20 and 30 (2-3%) boys will suffer a surgical complication, and another 2 to 3 (0.2-0.3%) will suffer a more serious complication.
The really curious statistic is the last in each group. About 10 (~1%) babies may need to have the circumcision done again due to a poor result. If normal, healthy boys are left with their normal, healthy foreskin, 10 (1%) of them will need a medically-necessary circumcision later in life. Those numbers look curiously similar.
So, to recap the facts in this context, circumcision is the permanent removal of a normal, healthy foreskin from a boy who can’t offer his consent to eliminate the 1% lifetime risk that he’ll need a circumcision.
There are other potential benefits, which Mr. Stern links in great detail. I have no problem including them, regardless of how weak or stupid I think they may be. That still isn’t enough to permit non-therapeutic child circumcision. The inputs into the decision are facts, but their value is not. Each person is an individual with his own preferences that his parents can’t know. What Mr. Stern values is not automatically what I value. Or to make the more appropriate connection, what parents value is not automatically what their son will value. That is why proxy consent requires a stricter standard than consent. A surgical decision that permanently alters a healthy child’s body can’t be permitted within proxy consent.
Mr. Stern writes this curious statement among many curious statements:
… Yet in the past two decades, a fringe group of self-proclaimed “intactivists†has hijacked the conversation, dismissing science, slamming reason, and tossing splenetic accusations at anyone who dares question their conspiracy theory. …
What a specific subset of people do is hardly the entirety of the argument or proof in favor of his position. Again, this is just silly, indefensible ad hominem. But what he says is also untrue. Dismissing science? Not here. I’ll accept any claimed benefit. The argument against forcing circumcision on a child is still as powerfully conclusive. Slamming reason? Stating that normal, healthy children should not undergo surgery is the position using reason. Conspiracy theory? Nope. Parents who circumcise, and people who support that option, are generally well-intentioned. I can show examples where that isn’t true, but I’m aware that such evidence is isolated. It’s surely true that some doctors circumcise for the money. I assume most circumcise because they believe it’s acceptable or believe parents should choose, even if the doctor wouldn’t. It’s important to understand how we got here, but I don’t much care about placing blame for that. I care about moving forward. There are any number of like-minded individuals Mr. Stern could find and talk to rather than write the wrong things he wrote.
… For doctors, circumcision remains a complex, delicate issue; for researchers, it’s an effective tool in the fight for global public health. But to intactivists, none of that matters. …
All of that matters. No one I know believes that adult (or older teen) males shouldn’t be able to volunteer for non-therapeutic circumcision.
Mr. Stern’s tactic here is what he’s complaining about. It’s similar to when Dr. Amy Tuteur goes on a tedious rant about “foreskin fetishists”. Smear your opponents because they smear you. “They”, of course. Internet comments are a part of humanity, not representative of it.
… The first rule of anti-circumcision activism, for instance, is to never, ever say circumcision: The movement prefers propaganda-style terms like male genital cutting and genital mutilation, the latter meant to invoke the odious practice of female genital mutilation. (Intactivists like to claim the two are equivalent, an utter falsity that is demeaning to victims of FGM.)
I’ve written circumcision a whole bunch above. But circumcision is genital cutting, because facts. The comparison is in the principle of those facts. Non-therapeutic genital cutting on a non-consenting individual is unethical. It’s also genital mutilation if we are to accept the WHO definition of female genital mutilation:
Female genital mutilation (FGM) comprises all procedures that involve partial or total removal of the external female genitalia, or other injury to the female genital organs for non-medical reasons.
…
… It is nearly always carried out on minors and is a violation of the rights of children. The practice also violates a person’s rights to health, security and physical integrity, the right to be free from torture and cruel, inhuman or degrading treatment, and the right to life when the procedure results in death.
The issue is human rights, not a specific subset of human rights from which male minors are somehow exempt.
Anti-circumcision activists then deploy a two-pronged attack on some of humanity’s most persistent weaknesses: sexual insecurity and resentment of one’s parents. Your parents, you are told by the intactivists, mutilated you when you were a defenseless child, violating your human rights and your bodily integrity. Without your consent, they destroyed the most vital component of your penis, seriously reducing your sexual pleasure and permanently hobbling you with a maimed member. Anti-circumcision activists craft an almost cultic devotion to the mythical powers of the foreskin, claiming it is responsible for the majority of pleasure derived from any sexual encounter. Your foreskin, intactivists suggest, could have provided you with a life of satisfaction and joy. Without it, you are consigned to a pleasureless, colorless, possibly sexless existence.
Some take that approach. I only speak for myself on being unhappy with circumcision. I’ll quote myself on his generalization:
… The problem is not that circumcision is bad, per se. Healthy men who choose to have themselves circumcised are correct for their bodies. Men circumcised as infants who are happy (or indifferent) about being circumcised are also correct for their bodies. …
But if you only dive into comments sections, it’s easy to believe that’s the only opinion. It’s not excusable to believe that, but it’s easy.
Intactivists gain validity and a measure of mainstream acceptance through their sheer tenacity. Their most successful strategy is pure ubiquity, causing a casual observer to assume their strange fixations are widely accepted. Just check the comment section of any article pertaining to circumcision. …
Ahem.
Take, for example, the key rallying cry of intactivists: That circumcision seriously reduces penis sensitivity and thus sexual pleasure. …
My “key rallying cry” is that circumcision is medically unnecessary and violates the child’s basic rights to bodily integrity and autonomy. That holds up even if the rest of his paragraph’s citations hold up. Sexual satisfaction is a subjective evaluation to each individual. The ability to orgasm is not the full universe of sexual satisfaction. And any change to form changes function. The individual may view that change as good. He may view it as bad. Parents can’t know. That’s the ethical flaw in circumcising healthy minors.
… Study after …
Surely Mr. Stern read through the studies to understand exactly what they say. I have my doubts. I read it. That study is problematic when viewed as conclusively as Mr. Stern cites it. It requires nuance the study’s author provided. Does an appeal to authority sweep away any concerns about limitations?
… study after …
“Adult male circumcision does not adversely affect…” Is that proof that circumcision of male minors doesn’t affect sexual satisfaction, with the glaring caveat against surgery that such a male can’t know?
It’s also worth noting that Mr. Stern linked that same study again later in the paragraph. He also linked another study in consecutive sentences. And a third. That’s deceptive and improperly gives an impression about “an entire field of resarch”, no?
… ([No adverse effect] fits with what my colleague Emily Bazelon found when she asked readers for their circumcision stories a few years ago.) …
Ms. Bazelon’s premise and finding were ridiculous.
So much for circumcision’s supposedly crippling effect on sexual pleasure. But what about its effect on health? Intactivists like to call circumcision “medically unnecessary.” In reality, however, circumcision is an extremely effective preventive measure against global disease. …
The potential benefits don’t render non-therapeutic circumcision “medically necessary”. Earlier he complained about propaganda-style terms. Pretending that “medically unnecessary” doesn’t have an accepted, factual meaning is propaganda-style question begging.
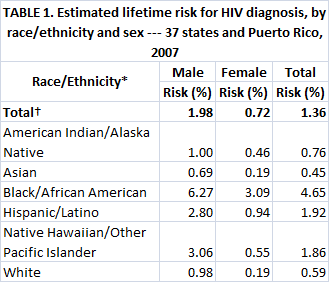
… Circumcision lowers the risk of HIV acquisition in heterosexual men by about 60 to 70 percent. … [ed. note: (Later in this paragraph, he uses the WHO link again.]
The “60” link states “male circumcision should be considered an efficacious intervention for HIV prevention in countries and regions with heterosexual epidemics, high HIV and low male circumcision prevalence.†Not one of those three criteria matches a Western nation. Those studies also involved adult volunteers, not unconsenting minors.
As both a personal and public health matter, circumcision is clearly in men’s best interest. …
Ethically, as a personal health matter, each healthy individual should decide for himself what body alterations are in his best interest based on his own preferences.
… Anyway, to intactivists, mutilation is mutilation; what does it matter if it’s for the greater good?
“The greater good” doesn’t matter because individuals are humans with rights, not statistics to be treated without regard for what they need or want. Life is full of risks. Because we seemingly can mitigate that does not mean we may or should.
{kind=link}