You’re having a baby. It’s a joyous event. You’re excited and unsure if you’re up to the task. There will be a lot of on-the-job learning, as well as mistakes that will be more amusing with the passing of time. You’re not supposed to have all the answers, and with experience, it will be clear you can’t plot them all in advance. The discovery is part of the process that makes parenting so exciting and strange and human.
Strangely, we assume parents should make a choice on circumcision if their baby is a boy. Our culture declares that the decision is for the boy’s parents. I’m asking you to make a choice against circumcision because it’s not a choice parents should make for their healthy son(s). Rightly considered, the choice belongs to the individual, not his parents. He should retain his choice absent some medical need for which circumcision – the most radical intervention – is the only available solution.
There are numerous reasons to reject circumcision for your healthy newborn son. The easiest summary comes from a basic principle and an economics concept. First, the principle: non-therapeutic genital cutting on a non-consenting individual is unethical. The problem is not that circumcision is bad, per se. Healthy men who choose to have themselves circumcised are correct for their bodies. Men circumcised as infants who are happy (or indifferent) about being circumcised are also correct for their bodies. But when circumcision is performed on a male without immediate medical need or his consent, there is no guarantee he will be happy with his parents making his choice. That’s the economic concept. All tastes and preferences are subjective and unique to the individual. The boy may like being circumcised, but he may not. It’s impossible to know which a son will prefer.
As the decision is commonly framed in America, circumcision is a referendum on the father’s penis and should be performed on his son if dad is circumcised so that their genitals match. The assumption is that, if it’s good enough for dad, it’s good enough for his sons. However, we know more now than we did when dad was born. We know that circumcision, being surgery, inflicts some guaranteed amount of harm by removing the foreskin and possibly the frenulum, as well as leaving a scar. There is also the possibility of complications inherent in every circumcision. Adhesions, skin bridges, bleeding, infection, greater-than-expected damage to the penis, and worse are all possibilities. Aesthetic symmetry between father and son is insufficient to justify surgery on a child. Rejecting circumcision for a son is sensible, not a referendum on the quality or functionality of his father’s penis.
When those inherent risks are considered, they’re often discussed as a minor trade-off for the potential benefits. The problem is that infant circumcision is almost always non-therapeutic. There is no malady to be resolved, no objective trade-off to be made. Every benefit supposedly in favor of circumcision involves something that might happen or might be desired by the individual. It’s an aggressive intervention on a healthy child whose foreskin will likely remain healthy throughout his life.
Every potential benefit from circumcision can be achieved through less invasive methods that prevent or treat the uncommon ailments cited. Many of these methods, such as condoms, are still required after circumcision. In the unlikely situation where the child eventually requires intervention, a doctor up-to-date on treating an intact penis will still likely be able to resolve a foreskin problem without circumcision. Should circumcision be necessary, he will experience some pain. Leaving him intact does not guarantee that he will eventually experience this pain. Circumcising him when he’s healthy guarantees he will experience pain. The choice is imposing pain that he will feel or exposing him to risk that he might experience pain later. The latter involves pain that he’d likely be able to ameliorate with pain management that an infant can’t have. Even if we assume there is no pain during the procedure, there will be pain during the healing process. Add to that the presence of urine and feces in repeated contact with a healing wound, and the choice to wait until it might be necessary becomes clearer.
For the claimed medical benefits, I accept all of them as possible, even where, for example, I believe there may be flaws in the methodology of the relevant studies. The analysis still leads to the same conclusion if all benefits are assumed to be possible. The details of each matter against circumcision and reveal their flaws. When considered in context, the proposed benefits are weak compared to the availability of prevention methods and treatments both more effective and less invasive than prophylactic circumcision. As Dr. Morten Frisch et al state (pdf), the “cardinal medical question should not be whether circumcision can prevent disease, but how disease can best be prevented.”
To illustrate the weakness of the proposed benefits, consider two commonly cited potential benefits: UTIs and HIV. The benefit for UTIs is a risk reduction from 1 percent of boys in the first year of life to between .1 and .3 percent of boys in the first year of life. Even for the intact boys, this risk is already significantly less than it is for girls. Most UTIs are easily treated without surgery. The same treatments that work for girls also work for boys.
The Canadian Pediatric Society states that, within every 1,000 circumcised boys, two will be admitted to the hospital for a UTI before their first birthday. Within every 1,000 boys left with their foreskins, seven will be admitted to the hospital for a UTI before their first birthday. Factor in the circumcised boys who will need some further treatment for complications, and the risks become clear. Circumcision can cause more problems than it seeks to prevent. As the CPS states, of the 1,000 boys who keep their foreskins, only ten of them “will have a circumcision later in life for medical reasons”. Prophylactic circumcision to avoid a one percent risk of needing that circumcision later is odd.
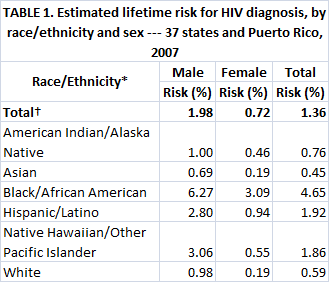
For the reduced risk of HIV, there are several significant problems related to non-therapeutic child circumcision. This potential benefit has only been found for female-to-male transmission in high-risk populations, and the studies only looked at voluntary, adult circumcision. None of those three aspects describes the situation in the United States or other first world nations. Our sexually transmitted HIV epidemic is male-to-male, and circumcision has not been shown to have any benefit there. Further, the relative risk reduction from circumcision for female-to-male transmission in the U.S. is an estimated 15.7%, far less than the often-cited 60% relevant to Africa. The absolute lifetime risk of HIV infection is already low in the United States. The lifetime absolute risk reduction is small. This summarized table provides the details. And what will science know about preventing or curing HIV by the time a child born today is sexually active?
As stated before, condoms are still necessary after circumcision. Circumcision doesn’t change the male’s required sexual behavior. Parents retain their responsibility to teach him the importance of safe sex practices (and proper hygiene techniques). Nor is there proof that infant circumcision has the same benefits found for voluntary, adult circumcision. Apart from research on UTIs, the potential benefits have been found only in studies using adult volunteers. Despite both being “male circumcision”, the two are not quite the same surgery. The significant difference in consent is most critical, but the foreskin hasn’t separated at birth and must be forced free from the rest of the penis to circumcise an infant. This introduces additional physical trauma and risks for an infant.
The proposed cultural benefits suffer under examination, as well. He has his normal genitals? Women won’t date him, or his peers will make fun of him, the thinking goes. We forget to consider whether he’d prefer his foreskin more than a partner who requires him to be circumcised or if he’ll even encounter a partner who prefers circumcision¹. Parents can build enough self-worth into their children to withstand teasing. That’s essential because children will always find something about their peers to tease. If it’s not his foreskin, it’ll be his height or hair color or clothing or whatever else is easy. Anyway, the locker room fear is rooted in the experiences of prior generations when communal showering was common in schools. It’s best examined in the present rather than holding to a scenario that no longer exists, especially as fewer parents circumcise their sons. Half or more of his peers will be intact. If he is “different”, he’ll be different like many of his peers. As children grow, parents realize their goal is not to teach their child to conform, but rather to help him become an independent person whose differences make him who he is. Making a major, irreversible decision for him before parent and child have grown to that point in their relationship may become something the parent or the child regrets.
The premise of this approach is “I don’t know”. None of us knows. We don’t know what we’ll want in the future. We don’t know what science will discover that makes circumcision even more unnecessary to achieve the possible benefits. We don’t know who we’ll be or who we’ll meet. Not circumcising sons in the absence of medical need prioritizes optimism over unfounded fear. It’s about keeping their choices open until they can express their personal preference about what they want and what will make them happy. It’s a realization that “what if” can be about a good future rather than succumbing to a fear of unlikely dangers.
Your son will be born with a foreskin. His prepuce is normal. It will belong to him, just like every other normal part of his body. It has functions. You want what is best for your children. Your son can always have his foreskin removed later, either for need or choice. He can’t put it back if he wants it after circumcision. Choosing to leave your son intact is the better choice.
¹ Many non-Americans are flabbergasted when they learn that circumcision has been so prevalent in the U.S. Their primary experience is with men who still have their foreskins. Given the declining rate of circumcision, the future American partners of a child born today will likely mirror that acceptance.
{kind=link}