This almost-good post from the AHA Foundation, FGM is Not Female Circumcision, and Other Thoughts on Terminology, is worth discussing for the reason it is not good.
The premise that female genital mutilation (FGM) is not “female circumcision” is correct. Language matters. In basic semantics, calling FGM “circumcision” is inaccurate. The etymology of the word circumcision means “to cut around”. That can be done to the female prepuce, in a sense, but that’s not how we understand it. I’m willing to grant this, and the result that the term circumcision doesn’t apply to females.
The gist of the AHA Foundation’s post is about the ethical implications from terminology:
A number of organizations and advocacy groups refer to the procedure as “female genital cuttingâ€, or “FGM/C†to encompass both terms. The argument for “cutting†instead of “mutilation†primarily hinges on the belief that mutilation implies malicious intent on the part of parents or the community, or is otherwise demeaning or insensitive to the cultural particularities of any group that performs FGM. Some argue that referring to it as cutting is a less provocative and more balanced term. Particularly when speaking with those who have undergone the procedure themselves or in reaching out to affected communities, we do see the value in using the more neutral terminology of “cutting†rather than “mutilationâ€, but otherwise believe it important to state clearly that the procedure is a form of abuse.
I agree with that. What is done to the healthy genitals of females without their consent in any form of FGM/C is morally and ethically wrong. It is indefensible. We must be clear that this violence is abuse. It should never be tolerated.
The AHA Foundation’s post fails because of its next-to-last paragraph.
The argument for referring to FGM as “female circumcision†is blatantly off-base. Female circumcision was the popular term until approximately the 1980s, when FGM and FGC came into usage. As mentioned above, to perform a procedure that parallels male circumcision, one would only remove the prepuce of the clitoris, something that is hardly ever done. (The prepuce is the “hood†or fold of skin that surrounds the clitoris and has no impact on sexual arousal or pleasure.) In nearly all cases, at minimum, either part or all of the clitoris, labia minora, labia majora is removed. To use the term “circumcision†to refer to what is happening to these girls minimizes the brutality of the procedure and ignores the fact that is an act of violence.
First, the paragraph is likely factually wrong when stating the clitoral hood has no impact on sexual arousal or pleasure. It’s bizarre that this made it into the post. I suspect the connection is an implication that the male prepuce also has no impact on sexual arousal or pleasure. Whether the clitoral hood affects arousal or pleasure, its removal would alter the woman’s sexual experience. That is a reason removing it without the individual’s consent is unethical. The parenthetical makes no sense.
To my point, since the post brought it up, what parallels male circumcision is not the only consideration. There are recognized forms of FGM/C less harmful than male circumcision. Much, if not all, of Type IV is comparable to or less harmful than a typical male circumcision. The stated, correct argument against FGM/C in the post (and elsewhere) is that any genital cutting on a female without need or her consent is wrong. (Including removal of the prepuce.) Any lesser conclusion or implication for male circumcision is moral relativism.
The paragraph’s flaw is its implication that FGM/C should not be called circumcision because circumcision is not a brutal act of violence. I doubt this is what the author means. I trust that the AHA Foundation recognizes that males possess the same “basic rights and freedoms” listed on its About page, including “security and control of their own bodies”. But the argument in that paragraph is predicated on minimizing a form of genital cutting, and based solely on gender. The general thrust of the debate is that FGM/C is often done with crude instruments in unsanitary conditions. It is. However, no one suggests that FGM/C performed in a hospital setting with clean instruments is somehow acceptable. At its core, cutting healthy genitals without the person’s consent is the issue.
The accurate approach would’ve been to leave out male circumcision and focus the paragraph accordingly. It would not be difficult. For example: “The term circumcision minimizes the brutality of genital cutting without need or the individual’s consent and ignores the fact that it is an act of violence.”
I do not believe those focused on ending FGM/C are required to actively advocate against male circumcision genital cutting. I expect them not to state or imply that male genital cutting without need or consent is acceptable. I expect them not to do this, from an exchange that started with the bottom tweet¹:
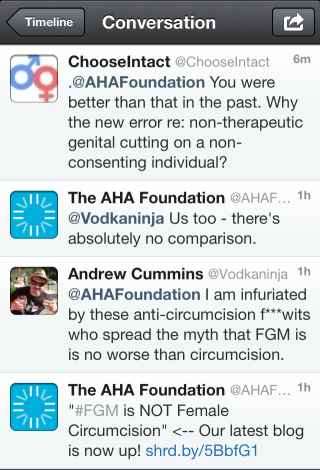
They responded to me:
We’re not advocating for anyone to be cut, only trying to point out the severity and harm done with #FGM.
I recognize that, as I indicated. But the response to Mr. Cummins was incorrect. There is no excuse for saying something false. (Or following up in agreement to his ad hominem.)
An organization that carelessly ignores the broader foundational principle to its work deserves no credibility. Every point that rejects FGM/C in the post applies to male genital cutting. In the points where the severity between the two is almost always different, and radically so, that is a critical distinction I’ve highlighted before. But something that should inform punishment rather than legality should not be used so recklessly. FGM/C isn’t made less terrible just because generally less-severe male genital cutting violates the same principle. Yes, those against forced male genital cutting need to be responsible when interjecting into a discussion on FGM/C, including by doing so less often. The same need for responsibility holds true for those who advocate against FGM/C.
¹ Contrary to Mr. Cummins’ rant, the argument is that non-therapeutic genital cutting on a non-consenting individual is wrong. There is almost always a difference in the degree of harm imposed from male and female genital cutting. It is often significant. But as the information in the AHA Foundation’s post also demonstrates, there is no difference in kind.